

双侧游离股后内侧皮瓣移植再造单侧乳房的经验
宋达疆1 李赞1 章一新2
本文来源:《中华整形外科杂志》2023年2月 第39卷 第2期
DOI:10. 3760 / cma.j.cn114453-20220323-00083
作者单位:1湖南省肿瘤医院肿瘤整形外科, 长沙410008;2上海交通大学医学院附属第九人民医院整形外科, 上海200000李赞,Email:zzanli@163.com
通信作者:李赞,Email:zzanli@163.com
【摘要】
目的 探讨应用双侧游离股后内侧皮瓣再造单侧乳房中的技术要点和注意事项。
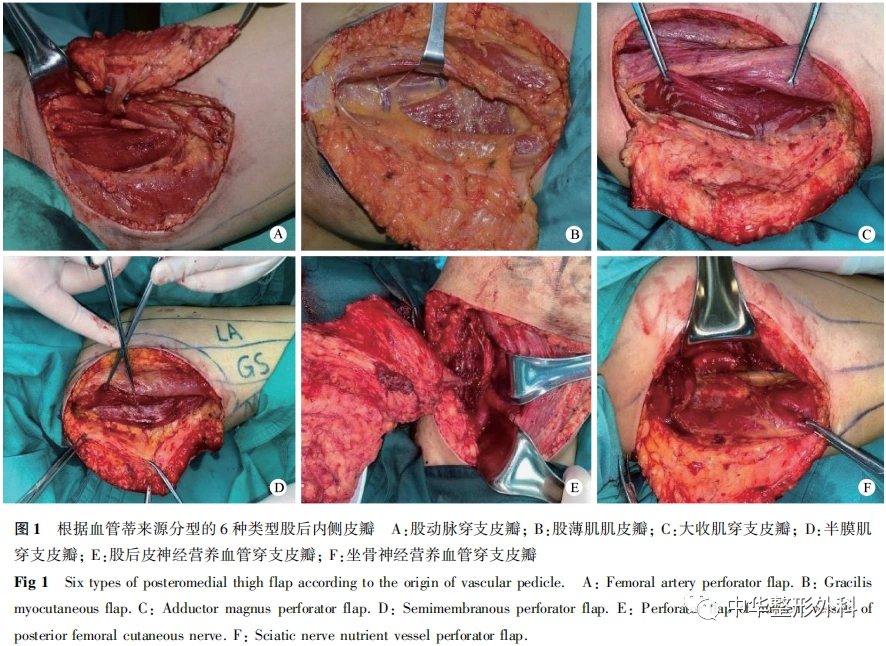
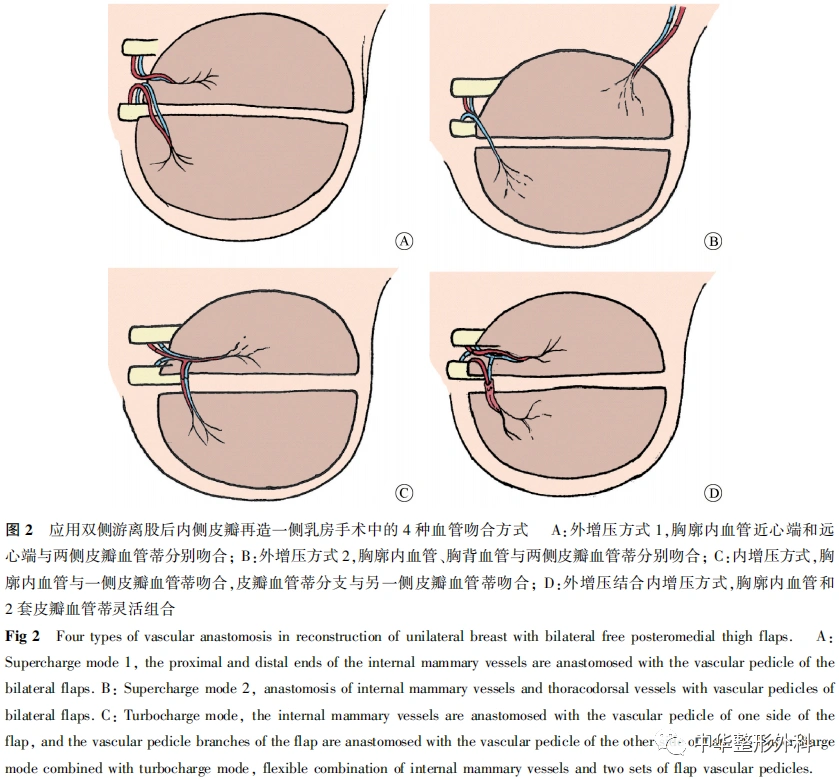
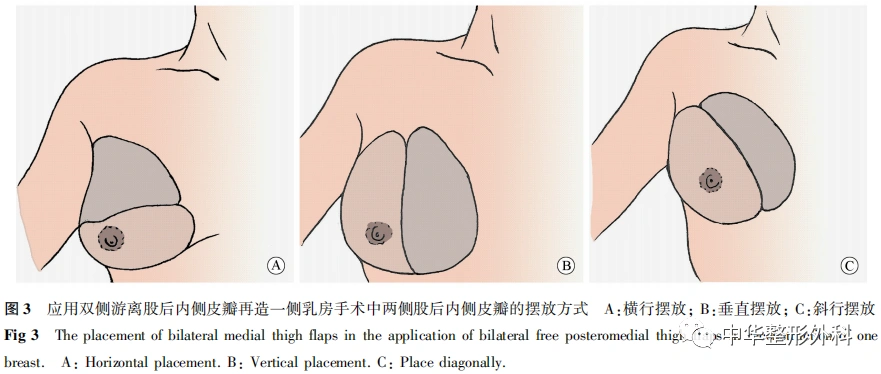
方法 收集2018年10月至2020年12月湖南省肿瘤医院肿瘤整形外科收治的乳腺癌改良根治术后行即刻或延期双侧游离股后内侧皮瓣移植再造一侧乳房患者的临床资料,进行回顾性分析。根据血管蒂来源,切取的股后内侧皮瓣包括6种类型:股动脉穿支皮瓣、股薄肌肌皮瓣、大收肌穿支皮瓣、半膜肌穿支皮瓣、股后皮神经营养血管穿支皮瓣、坐骨神经营养血管穿支皮瓣。血管吻合方式包括4种:(1)外增压方式1,胸廓内血管近心端和远心端与两侧皮瓣血管蒂分别吻合;(2)外增压方式2,胸廓内血管和胸背血管与两侧皮瓣血管蒂分别吻合;(3)内增压方式,胸廓内血管与一侧皮瓣血管蒂吻合,皮瓣血管蒂分支与另一侧皮瓣血管蒂吻合;(4)外增压结合内增压方式,胸廓内血管和2套皮瓣血管蒂灵活组合。两侧股后内侧皮瓣摆放方式包括3种:横行摆放、垂直摆放、斜行摆放。对术后皮瓣成活情况、再造乳房外形、供区瘢痕、对下肢功能的影响及乳腺癌复发情况进行随访。
结果 共纳入12例患者,年龄(37.4±3.6)岁(27~47岁)。肿瘤均为单侧,其中左侧7例,右侧5例;即刻乳房再造8例,延期乳房再造4例。术中共切取24块股后内侧皮瓣,包括:股动脉穿支皮瓣1块,股薄肌皮瓣6块,大收肌穿支皮瓣14块,半膜肌穿支皮瓣1块,股后皮神经营养血管穿支皮瓣1块,坐骨神经营养血管穿支皮瓣1块。血管吻合方式:外增压方式1有5例,外增压方式2有4例,内增压方式有2例,外增压结合内增压方式有1例。皮瓣摆放方式:横行摆放3例,垂直摆放4例,斜行摆放5例。皮瓣长(20.6±0.4) cm、宽(7.1±0.3) cm、厚(3.6±0.5) cm,血管蒂长度为(6.9±0.5) cm,动脉管径为(1.9±0.3) mm,静脉管径为(1.8±0.6) mm。皮瓣平均质量为245 g(165~415 g)。2例患者术中同时行健侧乳房缩乳上提术,2例同时行对侧乳房假体置入术。12例患者获随访6~18个月,平均10.5个月,所有皮瓣均成活,再造乳房外形可,弹性好,无皮瓣挛缩变形;皮瓣供区仅遗留线性瘢痕,对下肢功能无影响,患者对乳房外形满意,未出现乳腺癌复发病例。
结论 应用双侧游离股后内侧皮瓣移植再造单侧乳房相应采用的皮瓣形式、血管吻合方式和乳房塑形方式都较为灵活,需要灵活选择以确保手术安全、效果满意。该方法特别适用于下腹部组织量不足或者传统双侧血管蒂腹壁下动脉穿支皮瓣再造乳房外观难以满意的患者。
【关键词】乳腺肿瘤;股后内侧皮瓣;乳房再造
Experience of bilateral free posteromedial thigh flaps for unilateral breast reconstruction
Song Dajiang1, Li Zan1, Zhang Yixin2
1Department of Oncology Plastic Surgery, Hunan Cancer Hospital, Changsha 410008, China; 2Department of Plastic and Reconstructive Surgery, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200000, China
Corresponding author: Li Zan, Email: zzanli@163.com
【Abstract】
Objective To investigate the technical highlights and pitfalls in unilateral breast reconstruction with bilateral free posteromedial thigh flaps simultaneously.
Methods Clinical data of patients who received one-staged or delayed unilateral breast reconstruction with bilateral free posteromedial thigh flaps transplantation after modified radical mastectomy were collected and retrospectively analyzed, from October 2018 to December 2020 in the Department of Oncology Plastic Surgery, Hunan Cancer Hospital. There are six types of posteromedial femoral flap: femoral artery perforator flap; gracilis myocutaneous flap; magnus adductor perforator flap; semimembranous muscle perforator flap; posterior femoral cutaneous nerve nutrient vessel perforator flap; sciatic nerve nutrient vessel perforator flap. There are 4 types of vascular anastomosis: (1) supercharge mode 1, the proximal and distal ends of the internal mammary vessels were anastomosed with the vascular pedicle of the bilateral flaps; (2) supercharge mode 2, anastomosis of internal mammary vessels and thoracodorsal vessels with vascular pedicles of bilateral flaps; (3) turbocharge mode, the internal mammary vessels were anastomosed with the vascular pedicle of one side of the flap, and the vascular pedicle branches of the flap were anastomosed with the vascular pedicle of the other side of flap; (4) supercharge mode combined with turbocharge mode, flexible combination of internal mammary vessels and two sets of flap vascular pedicles. There are three ways to place the posteromedial thigh flaps: horizontal placement; vertically placement; obliquely placement. The survival of the flaps, the shape of the reconstructed breast, the scar in the donor area, the influence on lower limb function and the recurrence of breast cancer were followed up.
Results A total of 12 patients were included, with a mean age of 27 to 47 years (mean 37.4±3.6). 7 cases on the left and 5 cases on the right. There were 8 cases of one-staged breast reconstruction and 4 cases of delayed breast reconstruction. A total of 24 medial thigh flaps were harvested, including femoral artery perforator flap in 1 case, gracilis myocutaneous flap in 6 cases, magnus adductor perforator flap in 14 cases, semimembranous muscle perforator flap in 1 case, posterior femoral cutaneous nerve nutrient vessel perforator flap in 1 case, and sciatic nerve nutrient vessel perforator flap in 1 case. Vascular anastomosis mode included: supercharge mode 1 in 5 cases; supercharge mode 2 in 4 cases; turbocharge mode in 2 cases; supercharge combined with turbocharge in 1 case. The flap placement method included: horizontal placement in 3 cases, vertically placement in 4 cases and obliquely placement in 5 cases. The length of flap was (20.6±0.4) cm, width was (7.1±0.3) cm and thickness was (3.6±0.5) cm. The length of vascular pedicle was (6.9±0.5) cm, the diameter of artery was (1.9±0.3) mm and the diameter of vein was (1.8 ± 0.6) mm. The average weight of the flap was 245 g (165-415 g). Two cases underwent mastopexy on the ipsilateral side, and two cases underwent contralateral breast prosthesis implantation immediately. All flaps survived totally. All 12 patients were followed up for 6-18 months (10.5 months on average) with satisfied result. The reconstructed breasts’ shape, texture and elasticity was good and no flap contracture deformation happened. Only linear scar left in the donor sites, the function of thighs was not affected. No local recurrence happened.
Conclusion The method of flap harvestion, vascular anastomosis and breast shaping in applying bilateral free posteromedial thigh flaps for unilateral breast reconstruction are flexible, need to be selected flexibly to ensure the safety and satisfaction of the outcome. It is especially appropriate for patients with insufficient tissue in the lower abdomen or with unsatisfactory appearance of breast reconstruction with traditional bilateral vascular pedicle deep inferior epigastric artery perforator flap.
【Key words】Breast neoplasms; Posteromedial thigh flap; Breast reconstruction
Disclosure of Conflicts of Interest: The authors have no financial interest to declare in relation to the content of this article.
Ethical Approval: Ethical approval was given by the Medical Ethics Committee of Hunan Cancer Hospital(201701)
自体乳房再造具有其独特的优势,随着乳腺肿瘤整形外科的不断发展,越来越多的技术可以使自体乳房再造获得更加满意的效果,对身体的损伤程度也进一步减少[1,2,3]。虽然下腹部皮瓣是自体乳房再造的金标准,但是在中国女性人群中,相当一部分乳腺癌患者偏消瘦,腹部并没有足够的皮肤和皮下组织可利用,难以达到较为满意的乳房再造效果,这也是自体乳房再造选用下腹部皮瓣作为乳房再造供区的禁忌证之一[4,5]。大腿内侧区域皮肤、皮下组织质地较好,组织量较为丰富,血管解剖较为稳定,血运来源多样,也是较为理想的皮瓣供区[6,7,8,9]。其主要缺点是单纯一侧股后内侧皮瓣所能提供的皮肤和皮下组织量难以完成乳腺癌改良根治术后乳房再造的需要[10]。而随着显微外科技术和组合皮瓣移植技术的不断发展,通过拼接两侧大腿内侧组织瓣,也可以获得满意的乳房外形效果[11,12,13]。之前已经有病例系列报道介绍双侧股后内侧皮瓣移植用于乳房再造[14,15],国内首篇这方面的病例报道也是由我们中心完成[16,17]。随着技术和经验的不断积累,我们发现采用组合双侧股后内侧皮瓣移植再造乳房可以获得较为满意的效果,而实际手术操作中制备皮瓣的解剖类型、血管吻合方法、皮瓣摆放方式及乳房塑形的技术要点都对术者的技术和经验要求较高。通过总结归纳并详细分类,我们初步制定了较为成熟的采用双侧股后内侧皮瓣移植完成一侧乳房再造的手术流程和应对方法。
资料与方法
一、资料选择
收集2018年10月至2020年12月湖南省肿瘤医院肿瘤整形外科收治的乳腺癌改良根治术后行即刻或延期双侧游离股后内侧皮瓣移植再造一侧乳房患者的临床资料,进行回顾性分析。纳入标准:原发肿瘤直径≤4 cm,或乳腺癌术后放、化疗后1年以上未复发者;患者要求乳房再造;乳房较大需要皮岛及皮下组织量较多,而腹部皮下脂肪较少或既往行腹部手术,不适合采用腹壁下动脉穿支皮瓣进行乳房再造;患者拒绝以腹部作为皮瓣供区;双侧股后内侧脂肪组织较多。排除标准:随访时间<6个月。
本研究经湖南省肿瘤医院伦理委员会批准(201701),所有患者及家属签署手术知情同意书。
二、手术方法
(一)皮瓣设计
术前常规行双侧大腿CT血管成像(computed tomography angiography,CTA)定位股后内侧穿支血管数量、位置及来源,并结合可听式多普勒仪进一步验证穿支血管位置、数量并标记。设计皮瓣上端的标记在臀沟下方1 cm处,下端标记位于上端标记下约7 cm处;皮瓣设计为横行或纵向。
(二)肿瘤切除、受区准备、皮瓣切取
患者取仰卧位,双侧髋关节外展屈膝位,全身麻醉后手术分2组同时进行。
对于拟行即刻乳房再造的患者,受区准备组行乳腺癌改良根治术,送快速冰冻切片报告切缘无癌后,重新消毒、铺巾。如果为延期乳房再造患者,则行胸壁瘢痕彻底松解术并广泛游离胸部腔隙,选择胸廓内血管作为一侧皮瓣受区血管,标记第2、3肋软骨肋间,术中切除再造乳房一侧的部分第3肋软骨,长度1.5~2.5 cm,充分显露胸廓内动脉;显露并长段分离胸外侧血管或胸背血管作为另侧皮瓣受区血管备用。
皮瓣组制备双侧游离股后内侧穿支皮瓣。根据乳房继发缺损面积、形状,设计切取双侧游离股后内侧皮瓣。沿皮瓣前方设计线切开皮肤至皮下组织浅层,向周围潜行游离尽量多携带皮下组织于皮瓣内,保留大隐静脉完整性,从前向后于深筋膜平面掀起皮瓣,显露合适的穿支血管后,逆行分离血管蒂至接近发出平面,完全掀起皮瓣,结扎离断血管蒂后将皮瓣用肝素盐水纱布包裹并转移至乳房缺损区域。
根据血管蒂来源,将股后内侧皮瓣分为6种类型(图1):(1)股动脉穿支皮瓣;(2)股薄肌肌皮瓣;(3)大收肌穿支皮瓣;(4)半膜肌穿支皮瓣;(5)股后皮神经营养血管穿支皮瓣;(6)坐骨神经营养血管穿支皮瓣。

(三)血管吻合及皮瓣塑形
将两侧皮瓣转移至乳房缺损区域后,根据受区实际皮肤缺损范围予以初步皮瓣去表皮。以4-0可吸收缝线间断缝合固定于受区,在显微镜下吻合血管,血管吻合方式包括4种(图2):外增压方式1,胸廓内血管近心端和远心端与两侧皮瓣血管蒂分别吻合;外增压方式2,胸廓内血管、胸背血管与两侧皮瓣血管蒂分别吻合;内增压方式,胸廓内血管与一侧皮瓣血管蒂吻合,皮瓣血管蒂分支与另一侧皮瓣血管蒂吻合;外增压结合内增压方式,胸廓内血管和2套皮瓣血管蒂灵活组合。
确认皮瓣血运良好后调整皮瓣摆放位置并塑形,适当修整皮瓣大小并彻底止血,再次确认血管蒂无迂曲扭转后,以4-0可吸收缝线间断缝合固定皮瓣于受区。两侧股后内侧皮瓣摆放方式包括3种(图3):横行摆放、垂直摆放、斜行摆放。受区留置3根负压引流管,创缘分层缝合。供瓣区予以彻底止血后,留置负压引流管,逐层缝合皮下、皮肤,无菌敷料覆盖。
(四)术后处理及随访
术后常规对症支持治疗。术后最初2 d每小时观察皮瓣血运1次,术后第4天起每4小时观察1次;术后第2天开始鼓励患者进行床上双下肢抬腿及髋、膝、踝关节屈伸活动以预防下肢深静脉血栓;术后第5天开始指导患者下床活动。根据引流液情况,乳房引流管术后5~7 d拔除,大腿引流管术后7~10 d拔除。对术后皮瓣成活情况、再造乳房外形、受区和供区瘢痕、对下肢功能的影响及乳腺癌复发情况进行随访。
三、统计学处理
采用描述性方法进行统计学分析,正态分布计量资料以x
±s表示。
结 果
......
中华整形系列讲读|开播啦
11
第十一期内容
中国汉族人筛骨垂直板三维解剖测量
点击链接
成为讲者
“中华整形系列讲读会”讲者报名表

长按识别二维码关注视频号
观看更多精彩内容
微信视频号|中华整形外科
中华整形外科杂志
2023年 ▶▶▶
期刊官网:http://zhzxwkzz.yiigle.com
2023年每期35元,共12期,全年420元。
邮局订阅:可在全国各地邮政局订购,邮发代号80-855
网上订阅:中华医学会杂志社菁医汇商城
网址:http://jingyihui.org/shop/product/show/0/2253.html
电话:010-51322386
微信订阅:直接扫描下方二维码(手机端长按识别进入),订阅全年各期或选择性订阅某期《中华整形外科杂志》

过刊购买:中华医学会杂志社菁医汇商城,网址:http://jingyihui.org/shop/product/show/0/2253.html
目前可购买的过刊期有:目前可购买的过刊期有:2020-2022年1-12期. 电话:010-51322386


投稿方法:登录中华医学会网站http://cmaes.medline.org.cn,进行注册。注册成功后,申请成为《中华整形外科杂志》作者,即可投稿。如有问题,请致电:010-53968262。




推荐阅读
双侧游离股后内侧穿支皮瓣再造一侧乳房
游离腹壁下动脉穿支皮瓣在双侧乳房再造中的应用
腹壁下动脉穿支皮瓣移植乳房再造术中与胸廓内血管吻合方式的选择
原创文章,作者:中华整形外科,如若转载,请注明出处:https://www.meiye.net/191263.html