

应用Ilizarov技术治疗创伤后下肢短缩伴马蹄内翻足
徐明亮1 陈国梁1 董长红1 彭爱民2 石荣剑1 伊力扎提·伊力哈木1
本文来源:《中华整形外科杂志》2023年3月 第39卷 第3期
DOI:10. 3760 / cma.j.cn114453-20220531-00169
作者单位:1徐州仁慈医院骨科, 徐州221004; 2北京骨外固定技术研究所, 北京100041
通信作者:石荣剑,Email: minyexu@126.com
【摘要】
目的 探讨应用Ilizarov技术治疗创伤后下肢短缩伴马蹄内翻足的临床效果。
方法 回顾性分析2013年1月至2020年4月徐州仁慈医院骨科应用Ilizarov技术治疗的创伤后下肢短缩伴马蹄内翻足患者的临床资料。依据Ilizarov外固定穿针原则于患肢安装环形外固定架。术后3 d,以2 mm/d的速度调节足内、外侧螺纹杆,逐渐矫正马蹄内翻足;术后7 d,以1 mm/d的速度行小腿延长;马蹄内翻足矫正,继续佩戴外固定架维持4~6周,然后拆除足部固定架,配置足部支具固定6~8周;下肢长度恢复、延长处矿化良好后拆除小腿固定架。将术前及末次随访时记录的双下肢长度、距跟角度、踝关节跖屈和背伸角度、踝关节活动度进行对比;末次随访时用国际马蹄足畸形研究会(ICFSG)评分系统对患足进行评分和评级,分为优、良、中、差4级。应用SPSS 25.0软件进行统计分析,各测量指标数据及ICFSG评分以x±s表示,术前与术后末次随访数据比较采用配对t检验,P<0.05为差异有统计学意义。
结果 共纳入31例患者,其中男17例,女14例;年龄15~18岁,平均16.5岁;右侧16例,左侧15例;下肢短缩45~75 mm,平均65 mm。术后外固定架固定时间为4.5~6个月,平均5个月,随访时间为22~28个月,平均25.5个月,患侧下肢长度恢复,外形基本满意,恢复跖行步态。末次随访时与术前比较,患者足部前后跟距角(23.0°±2.1° vs. 8.5°±2.6°)、外侧距跟角(27.0°±4.3° vs. 11.2°±4.4°)、踝关节跖屈角度(24.5°±6.8° vs. 51.1°±6.5°)、踝关节背伸角度(5.8°±3.5° vs. -46.8°±7.0°)、踝关节活动度(30.3°±8.2° vs. 4.2°±1.6°)差异均有统计学意义(P均<0.01);ICFSG评分:末次随访时[(8.0±4.2)分]明显低于术前[(41.9±5.3)分](P<0.01),其中18例为优,9例为良,4例为中。2例后期出现畸形复发,二期行距舟关节和跟骰关节融合、胫后肌腱前置术后,效果满意;4例出现足趾挛缩畸形,在足趾处行趾长屈肌腱松解后,未再复发;5例出现踝关节前方撞击症状,行关节镜下骨赘磨除后好转;6例患者下肢延长到位后拆除外固定架更换髓内钉行走;7例出现钉道感染,经更换固定针、钉道换药后好转。
结论 应用Ilizarov技术治疗创伤后下肢短缩伴马蹄内翻足,具有创伤小、畸形矫正动态可控等优点,可获得较好的效果。
【关键词】伊利扎罗夫技术;下肢短缩;马蹄足畸形;创伤
基金项目: 徐州市卫生健康委科技项目(XWKYHT20200022)
Application of the Ilizarov technique in the treatment of post-traumatic lower extremity shortening with talipes equinovarus
Xu Mingliang1, Chen Guoliang1, Dong Changhong1, Peng Aimin2, Shi Rongjian1, Yilizati·Yilihamu1
1Department of Orthopaedics, Xuzhou Renci Hospital, Xuzhou 221004,China; 2Beijing Rehabilitation Hospital Affiliated to Capital Medical University, Beijing 100041, China
Corresponding author: Shi Rongjian, Email: minyexu@126.com
【Abstract】
Objective To investigate the effect of the Ilizarov technique in the treatment of post-traumatic lower extremity shortening with talipes equinovarus.
Methods Clinical data of patients with post-traumatic lower extremity shortening and talipes equinovarus treated by the Ilizarov technique in the Department of Orthopaedics of Xuzhou Renci Hospital from January 2013 to April 2020 were retrospectively analyzed. The annular external fixator was installed on the affected limb according to the Ilizarov principle of external fixation. 3 days after the operation, the internal and lateral screw rods were adjusted at the speed of 2 mm/d to gradually correct the talipes equinovarus. 7 days after surgery, the lower leg was lengthened at a speed of 1 mm/d. After the foot was corrected, the foot external fixator was continued to be worn for 4 to 6 weeks, and then the fixator was removed and the foot was immobilized with a brace for 6 to 8 weeks. The lower leg fixator was removed after the lower extremity length was restored and the bone mineralization at the extension site was good. The length of both lower extremities, angle of talonavicular joint, angle of plantar flexion and dorsal extension of the ankle, and range of motion of ankle were compared before surgery and at the last follow-up. At the last follow-up, the affected feet were scored and rated using the International Clubfoot Study Group (ICFSG) scoring system, which was divided into four grades: excellent, good, medium, and poor. SPSS 25.0 software was used for statistical analysis, and each measurement index and ICFSG score were expressed in Mean±SD. Paired t-test was used to compare the preoperative and last follow-up data, and P<0.05 was considered statistically significant.
Results A total of 31 patients were enrolled, including 17 males and 14 females. The age was 15-18 years old, with an average of 16.5 years old. There were 16 cases on the right side and 15 cases on the left side. The lower extremity shortening was 45-75 mm, with an average of 65 mm. The fixation time of the external fixator was 4.5-6 months after surgery, with an average of 5 months, and the follow-up time was 22-28 months, with an average of 25.5 months. The length of the affected lower extremity recovered, the shape was basically satisfactory, and the plantar gait was restored. At the last follow-up, compared with the preoperative period, the anteroposterior talocalcaneal angle of the foot (23.0°±2.1° vs. 8.5°±2.6°), from lateral talocalcaneal angle the foot (27.0°±4.3° vs. 11.2°±4.4°), ankle plantar flexion angle (24.5°±6.8° vs. 51.1°±6.5°), ankle dorsiflexion angle (5.8°±3.5° vs. -46.8°±7.0°) and ankle range of motion (30.3°±8.2° vs. 4.2°±1.6°) were statistically significant (P <0.01). ICFSG score: The points at the last follow-up (8.0 ± 4.2) were significantly lower than that before the operation (41.9 ± 5.3) (P<0.01), of which 18 were excellent, 9 were good, and 4 were medium. Two cases had recurrent deformities in the later stage, and the results were satisfactory after the fusion of the talonavicular joint and calcaneocuboid joint and the anteposition of the posterior tibial tendon in the second stage. There were 4 cases of toe contracture deformity, which did not recur after the release of the flexor digitorum longus tendon at the toe. Anterior ankle impingement was observed in 5 cases and improved after the arthroscopic osteophyte removal. After the lower extremity extension was in place, the external fixator was replaced by the intramedullary nail for walking in 6 patients. The infection of the nail path occurred in 7 cases, which improved after replacement of fixing pins and dressing change of the nail path.
Conclusion The application of the Ilizarov technique in the treatment of post-traumatic lower extremity shortening with talipes equinovarus has the advantages of small trauma and dynamic control of deformity correction, which can achieve good result.
【Key words】Ilizarov technique; Shortening of the lower extremity; Talipes equinovarus; Trauma
Fund program: Science and Technology Project of Xuzhou Municipal Health Commission (XWKYHT20200022)
Disclosure of Conflicts of Interest: The authors have no financial interest to declare in relation to the content of this article.
Ethical Approval: Ethical approval was given by the Medical Ethics Committee of the Xuzhou Renci Hospital(XZRCLL-LW-202302003).
在青少年时期,小腿创伤后瘢痕挛缩会影响小腿及足的发育[1],继发性出现下肢短缩及马蹄内翻足畸形。马蹄内翻足畸形导致足部骨骼及关节处于异常的位置,行走时足部关节受到身体重量的挤压,增加了发生创伤性关节炎的概率。为了恢复下肢长度并能使足部放平行走,需要行下肢延长、软组织松解、小关节融合、楔骨部分切除等系列手术,过程比较复杂,皮肤血管神经损伤等并发症也明显增加,效果难以明确。Ilizarov等研究发现了张力-应力法则,其基本定义为"给活体组织稳定、持续、缓慢的牵拉,可刺激某些细胞组织的活跃与再生,生长方式与原细胞组织一致"[2]。根据此原理,应用Ilizarov技术治疗下肢不等长,矫正创伤性马蹄内翻足已被广泛认同[3,4]。本研究中,我们对应用Ilizarov技术治疗的创伤后下肢短缩伴马蹄内翻足患者的临床资料进行回顾分析,以探讨其临床效果。
资料与方法
一、资料选择
回顾性分析2013年1月至2020年4月徐州仁慈医院骨科收治的创伤后下肢短缩伴马蹄内翻足患者的临床资料。纳入标准:(1)下肢短缩、马蹄内翻足继发于外伤;(2)根据Dimeglio分型[5]踝关节畸形为Ⅲ、Ⅳ级;(3)下肢短缩<10 cm;(4)应用Ilizarov技术进行治疗;(5)随访时间≥22个月,资料完整。排除标准:(1)有精神疾病患者;(2)合并同侧股骨短缩患者。
本研究经徐州仁慈医院伦理委员会批准(XZRCLL-LW-202302003),患者家属均自愿签署科研同意书。
二、方法
(一)术前准备
术前常规拍摄双下肢负重全长正位X线片,通过PACS软件[通用电气(中国)医疗集团GE影像管理系统],将股骨头中心与胫骨远端中心进行连线,测量双侧下肢的长度;拍摄足部X线片,应用PACS软件在正位X线片上测量跟骨和距骨中轴线的夹角(Kite角),即前后跟距角,在侧位X线片上测量距骨轴线与跟骨距骨关节面的夹角,即外侧距跟角;用量角器测量踝关节背伸、跖屈角度及踝关节活动度。根据国际马蹄足畸形研究会(International Clubfoot Study Group,ICFSG)评分系统[6]对患足从形态特征(12分)、功能状况(36分)、影像学表现(12分) 3个方面进行评分,总分0~60分,0分为正常,分数越高提示足部功能越差。根据评分分为4个等级:(1)0~5分为优,足外形正常,无足跟部内翻及前足内收畸形,足能放平,步态正常;(2)6~15分为良,畸形基本矫正,踝关节活动好,足能放平,步态尚好,遗留轻微内翻及前足内收;(3)16~30分为中,形态较术前明显改善,足跟内翻或外翻及跖屈畸形程度较轻,步态尚可;(4)31~60分为差,形态及功能较术前无明显改善,仍有马蹄内翻畸形,跛行明显。术前对患者及家属进行心理辅导,告知治疗过程中的注意事项,以取得其配合。
(二)手术方法
1.软组织松解及V形截骨
患者取平卧位,在硬腰联合麻醉或全身麻醉下进行手术。在内踝水平、跟腱内侧纵行切开长5 cm的切口,打开腱膜,在跟腱上行Z形切断,将踝关节背伸,以2号聚脂不可吸收缝合线缝合肌腱,3号可吸收胶原蛋白缝合线缝合腱膜,0号慕丝线缝合皮肤切口。将前足背伸外展,使跖筋膜处于紧张状态,以11号尖刀片经皮肤从足底内侧切断紧张的跖筋膜,矫正部分高弓及内收畸形。在外踝下方取一弧形切口,起自跟骨结节中点,经趾伸肌起点,止于距舟关节处,游离腓骨长、短肌,向两侧牵拉,暴露跟骨外侧面、跗骨窦、距骨颈。在矢状位上,第一处截骨线从距骨颈起,经跟骨前部止于跟骰关节与跟骨结节连线中点;第二处截骨线从跟骨结节与跟骨后关节面后缘之间的中点起,止于跟骰关节与跟骨结节连线中点,两截骨线呈V形,根据畸形情况适当截除骨质,闭合截骨端并以2.0 mm克氏针进行固定。通过该截骨可矫正部分跟骨内翻、内旋、前足内收、跖屈畸形。
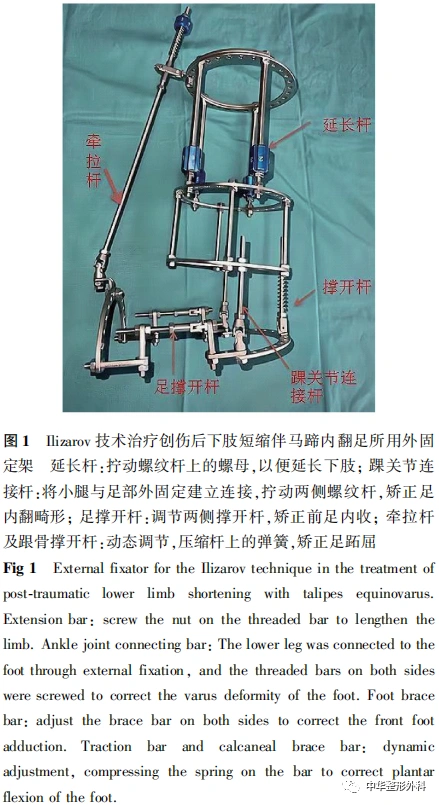
2.外固定架安装
外固定架(图1)由北京骨外固定技术研究所提供。根据患者小腿的直径选择合适孔径的环形架,小腿部外固定架由3个全环、4根螺纹杆组成,近端2个环之间为可伸缩的延长杆装置。在小腿远端和近端分别交叉打入2根直径2.5 mm的克氏针及1枚4.0 mm的Schanz钉,固定小腿部外固定架,穿针部位尽量避开瘢痕处,并确保固定针对皮肤软组织无张力。在胫骨结节下方1 cm处及腓骨中上段以"邮票边缘样"截断胫、腓骨。在踝关节两侧通过2根带铰链的螺纹杆与跟骨后侧的C形环连接,两侧铰链的连线为踝关节的活动轴。在跟骨C形环上通过跟骨中点横行打入1根直径2.5 mm的克氏针,在跟骨两侧与克氏针呈45°各打入1枚直径2.5 mm的Schanz钉。跟骨C形环与前足C形环通过带活动铰链的螺纹杆建立连接,通过第1跖骨及第5跖骨在前足横弓交叉打入2根直径2.0 mm的克氏针,固定于前足C形环上,在第1跖骨近段内侧辅助打入1枚直径3.5 mm的Schanz钉,固定于前足C形环上。最后在踝关节远端全环上与跟骨C形环后侧安装弹簧杆,前足C形环与小腿外固定架近端环连接带铰链的牵拉杆。用75%乙醇纱布缠绕钉道周围。

(三)术后处理
术后24 h内,静脉滴注抗生素,以预防感染,每天用75%乙醇消毒钉道。每天行膝关节、足趾主动和被动锻炼。术后3 d开始调节外固定架,首先调节踝关节两侧螺纹杆,每天撑开2 mm,共3 d,以增加踝关节间隙;然后只调节踝关节内侧螺纹杆,2 mm/d (分6次调节),逐渐矫正跟骨内翻畸形,同时调节前足两侧螺纹杆,2 mm/d(分6次调节),矫正前足内收。在此过程中同时调节前方带弹簧的牵拉杆与跟骨后侧带弹簧的撑开杆,5 mm/d(分10次调节),逐渐矫正跖屈畸形。前方牵拉杆、后方撑开杆动态松开,以便锻炼踝关节活动。术后7 d,以1 mm/d(分6次调节)的速度行小腿延长,结合小腿瘢痕的张力及钉道切割皮肤软组织情况,可对延长速度进行个性化调整,并让患者扶拐下床患肢负重行走。术后2周拍摄踝关节正、侧位X线片,观察踝关节间隙是否合适;拍摄胫腓骨正、侧位X线片,观察截骨延长处牵伸长度及骨痂生长情况。经过4~6周外固定的调节,马蹄内翻足已矫正,继续佩戴外固定架维持4~6周后拆除足部固定架,配置足部支具固定6~8周,去除足部支具后正常穿鞋行走。下肢长度恢复后8~12周,复查胫腓骨正、侧位X线片,观察延长处骨矿化良好后拆除固定架,并扶拐辅助行走6周。
(四)疗效评价
术后1、2、3、4、6、12、18、24个月门诊复查,拍摄双下肢负重全长正位X线片及足部正、侧位X线片。通过X线片测量双下肢长度差异、距跟角度;量角器测量踝关节跖屈、背伸角度,记录踝关节活动度,并对患者行ICFSG评分。
三、统计学分析
使用SPSS 25.0软件进行统计分析,各测量指标及ICFSG评分以x±s表示,术前与末次随访数据比较采用配对t检验,P<0.05为差异有统计学意义。
结 果
一、一般资料
......
中华整形系列讲读|开播啦
11
第十一期内容
中国汉族人筛骨垂直板三维解剖测量

长按识别二维码关注视频号
观看更多精彩内容
微信视频号|中华整形外科
中华整形外科杂志
2023年 ▶▶▶
期刊官网:http://zhzxwkzz.yiigle.com
2023年每期35元,共12期,全年420元。
邮局订阅:可在全国各地邮政局订购,邮发代号80-855
网上订阅:中华医学会杂志社菁医汇商城
网址:http://jingyihui.org/shop/product/show/0/2253.html
电话:010-51322386
微信订阅:直接扫描下方二维码(手机端长按识别进入),订阅全年各期或选择性订阅某期《中华整形外科杂志》

过刊购买:中华医学会杂志社菁医汇商城,网址:http://jingyihui.org/shop/product/show/0/2253.html
目前可购买的过刊期有:目前可购买的过刊期有:2020-2022年1-12期. 电话:010-51322386


投稿方法:登录中华医学会网站http://cmaes.medline.org.cn,进行注册。注册成功后,申请成为《中华整形外科杂志》作者,即可投稿。如有问题,请致电:010-53968262。





推荐阅读
Ilizarov技术治疗静脉畸形继发肢体挛缩
小腿后群肌内静脉畸形致马蹄足畸形原因分析及手术治疗
改良双翼皮瓣联合足底内侧皮片移植治疗先天性并指畸形
原创文章,作者:中华整形外科,如若转载,请注明出处:https://www.meiye.net/228816.html